What a difference a week makes! I am very pleased to report that many of the concerns so many raised at the hearing and in other venues about HB 3074 have been met and it is worthy of support as a true incremental improvement over existing law. The new Substitute Bill, which is not yet available online, can be
supported as an incremental improvement to the Texas Advanced Directives Act ("TADA").
Let’s jump right in and I will try to keep this as short as possible while still giving you bill text and
The original bill included the following exceptions to providing
artificially administered nutrition and hydration (“AANH”) read as follows:
SECTION 5. Section
166.046(e), Health and Safety Code, is amended to read as follows:
(e) If the
patient or the person responsible for the health care decisions of the patient
is requesting life-sustaining treatment that the attending physician has
decided and the ethics or medical committee [review process] has
affirmed is medically inappropriate treatment, the patient shall be
given available life-sustaining treatment pending transfer under Subsection
(d). This subsection does not
authorize withholding or withdrawing pain management medication, medical
procedures necessary to provide comfort, or any other health care provided to
alleviate a patient's pain. The
patient is responsible for any costs incurred in transferring the patient to
another facility. The attending
physician, any other physician responsible for the care of the patient,
and the health care facility are not obligated to provide life-sustaining
treatment after the 10th day after the written decision required under
Subsection (b) is provided to the patient or the person responsible for the
health care decisions of the patient unless ordered to do so under Subsection
(g), except that artificially administered nutrition and hydration must be
provided unless, based on reasonable medical judgment, providing artificially
administered nutrition and hydration would:
(1) hasten
the patient's death;
(2) seriously
exacerbate other major medical problems not outweighed by the benefit of the
provision of the treatment;
(3) result in
substantial irremediable physical pain, suffering, or discomfort not outweighed
by the benefit of the provision of the treatment;
(4) be
medically ineffective; or
(5) be
contrary to the patient's clearly stated desire not to receive artificially
administered nutrition or hydration.
(A note about reading draft
legislation: anything underlined is new text being added to existing law.
Anything crossed out in brackets is what current law says that is being removed
if this bill passes. Anything that is just plain text, no underline, no cross out, no brackets, is how the law reads currently.)
Those of us who opposed the original (and the first
Committee Substitute) bills were concerned about this very broad, subjective
language that allows for “quality of life" determinations to be the basis of withdrawing
care. That is what is called “passive euthanasia” and it happens here in Texas.
I described this in my prior post on HB 3074.
Today I received word that a compromise has been reached. The Agreement, which has already been publicized, is as follows:

Now, while I cannot link to the Substitute Bill because it is not yet online, I
can show you that this is how those exceptions now read:


In addition to Representative Tan Parker, others who helped Representative Springer are to be thanked: Representative Bryan Hughes (R-Mineola) who serves as the Pro-Life Whip in the Texas House, Representative James Frank (R-Wichita Falls), Representative Dan Huberty (R-Houston/Kingwood), Representative Stephanie Klick (R-Fort Worth), and Representative Richard Raymond (D-Laredo). We are very grateful for their diligence and time spent to facilitate changes to HB 3074.
The third exception is probably the most important change. The bill has gone from allowing the withdrawal of AANH when it the doctor believed it caused "discomfort" or "suffering" (which was not necessarily limited to only physical suffering since physical did not precede suffering, but only preceded pain, thereby opening the door to "quality of life" determinations) to requiring "substantial irremediable physical pain..."
The fourth exception was also problematic. Originally, it read "be medically ineffective" but that was open to many interpretations especially for a situation where, perhaps, the patient can assimilate food, but is otherwise, for example, dying of a terminal condition or is in a coma. A doctor could argue that the AANH is not medically effective - at reversing the underlying condition. This, too, could open the door for "quality of life" judgments. Now the language is very clear that it must be "medically ineffective in prolonging life." Of course, the withdrawal of AANH will almost always terminate life or hasten death faster even in someone who is otherwise afflicted with some serious illness or injury. This provides clarity.
Another amendment I like to the Committee Substitute is this paragraph (there was a version of it before, but it did not require the medical records, and, of course, the exceptions are more narrowly written now):

I like very much that the 10-day rush to find another facility does not begin until the medical records are provided. In the past, it has been difficult to get medical records in the short time given to transfer. I also like that this paragraph indicates that if a willing provider is found that treatment will continue past the 10 days.
Unfortunately, the law still allows for withdrawal of AANH and other life-sustaining care after the 10 days if a facility is not found. And, there is still only 10 days unless the facility just decides to give you more time, although you can still go to court and ask for more time (if you meet your burden there; it is not an automatic extension of time.)
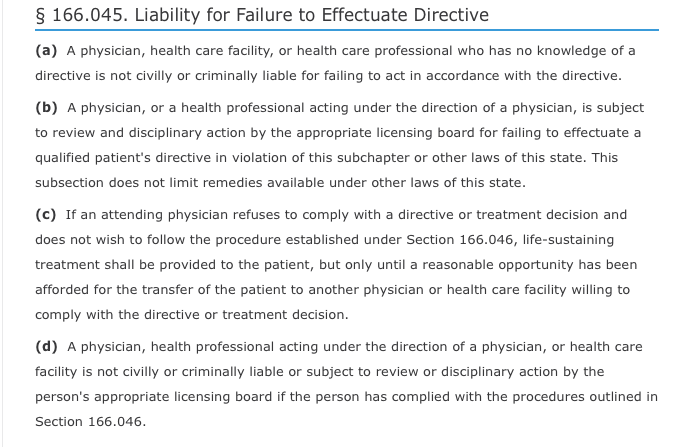
I expressed concerns about the lack of enforcement mechanism in the bill. That is not explicitly addressed in this particular bill. However, if the doctor or facility do not follow this procedure that HB 3074 amends, under Texas Health & Safety Code 166.045(d) they lose their immunity - which is the case under current law:
Under current law, there is a sparse process, medical records are hard to obtain, and there are no procedures for protecting a patient from the withdrawal of AANH or other life-sustaining treatments. It can be done for any reason, including "quality of life" reasons. While there was the potential for losing immunity under current law, there was not much in the way of protection that was afforded a patient that lent itself to being enforced.
Likewise, if the original exceptions had remained and had become law, they were open to so many interpretations that one could never really say that the procedure was not followed and the doctor or hospital could never lose immunity. Thus, there would be no enforcement mechanism.
Now, with these narrowly drawn exceptions that are not so open to just any interpretation and a deadline that does not start to run until medical records are obtained as part of the process under .046, I believe that there is an enforcement mechanism through a provision already in the law.
I confess that it is unclear to me, however, if non-compliance with Section 166.046 can be challenged during the process to request more time, if that could be a means to obtain more time, or if that would have to be a separately filed (and, hopefully, simultaneous) lawsuit. Sometimes the procedural aspects of new law take time to work out when they are not addressed in the law. Hopefully, this will not have to be used often, but I am glad that it is there just in case. There must always be checks and balances.
Either way, now there is a process to limit cases where AANH and other life-sustaining treatment are withdrawn against a patient's wishes. That combined with existing law mean a doctor and/or health care facility can be civilly and criminally liable for doing so if they do not follow the much more narrowly tailored process, including narrowly worded exceptions allowing for that withdrawal. That is, if this bill passes and becomes law.
I am very gratified that the recommendations of Texas Right to Life were used for these amendments. As said in the release:
While Texas Right to Life will continue to pursue patient protections and larger reforms to the Texas Advance Directives Act, limiting the circumstances in which food and water can be withdrawn is progress. Representative Springer considered our decade of experience as the only organization that helps patients and families facing futile care judgments; he heard our concerns and those of many others about the pitfalls of broad language, accepted our changes, and brought aboard the other stakeholders.
I have said before that Texas Right to Life is the only pro-life group that works to help patients navigate this process and has the most experience in the trenches. They know how the process works in reality and are in the best position to gauge what is real reform and how it would most likely be used versus what is merely aspirational.
UPDATE: The bill passed out of the State Affairs Committee this evening. It will now have to be brought up for a floor vote in the House. Of course, then it has to find its way to the Senate, be passed there, etc. It has a long ways to go.
There are still many problems with TADA that are not addressed by this bill, but it was always intended to be limited in its scope. I have detailed these problems in my prior posts and they were discussed in much of the testimony at the hearing on this bill. But I am so very happy to say that there is finally something that we can support as truly incremental improvement to TADA. This is an important step and I hope just the first of many, many more.
One final note, I really do think that all of you that testified against, called, and otherwise helped get the word out made a difference. It is no secret that these negotiations were hard. This is a very, very difficult issue. But some very big progress was made and that was no accident. So, thank you.
And, as always, thanks for reading!